Synoptic Overview Of Glue-Ear = Serous Otitis Media / Otitis Media With Effusion (OME)

Overview
Glue ear is one of the most common causes of hearing loss in children. It’s “silent” — no acute infection signs but fluid buildup behind the eardrum affects speech, learning, and balance.
What is OME?
Otitis Media With Effusion (OME) is the collection of non-infective fluid / mucus in the middle ear cleft for >3 months, with intact tympanic membrane. No fever, no pain. “ Glue” = thick, sticky mucoid effusion.
Figure 1
Anatomy of middle ear cleft
Epidemiology
1. Infants / Children: Peak 6 months – 7 years. ∼80% of kids have ≥1 episode by age 4. Boys > girls slightly. Higher in winter, daycare attendees.
2. Adults: Less common. When it occurs, think of Eustachian tube obstruction and rule out nasopharyngeal carcinoma.
Anatomical differences: Eustachian Tube
| Children | Adults |
|---|---|
|
|
Result:
Kids can’t ventilate / drain middle ear as well.
Causes of Eustachian Tube Dysfunction
1. Inflammation: Viral URTI, allergic rhinitis, adenoid hypertrophy
2. Obstruction: Adenoids hypertrophy, nasopharyngeal mass, cleft palate
3. Functional: Poor muscle function in Down’s, cleft palate, craniofacial syndromes
4. Pressure changes: Barotrauma from flying / diving
Pathophysiology + Role of Eustachian Tube
Functions of the Eustachian tube:
- Ventilates middle ear
- Drains secretions
- Protects middle ear of secretions from the nasopharynx.
Dysfunction leads to negative middle ear pressure, tympanic membrane retraction. There is also transudation of fluid from mucosa. Mucus glands hyperplasia increases fluid production and “glue” forms.
The fluid is viscous and gives poor sound conduction.
Tympanic Membrane Retraction and Sade classification:
Sade Classification for retraction of Pars Tensa:
Grade 1: Mild retraction but does not contact the incus, normal TM color
Grade 2: TM contacts long process of incus (adhesion is called tympano-incudopexy) or contacting stapes (adhesion is called tympanostapediopexy)
Grade 3: TM contacts promontory but not adhered to it
Grade 4: Atelectasis / adhesion to promontory. TM is adhered to the promontory.
Grade 5: 3 or 4 with perforation in the TM.
Tos Classification -Pars Flaccida Retractions: Used for TM retraction pockets.
Grade 1: Small attic dimple
Grade 2: Pars Flaccida retracted minimally and draped over neck of malleus
Grade 3: As grade 2 with erosion of outer attic wall (scutum).
Grade 4: Deep retraction with unresectable accumulated keratin.
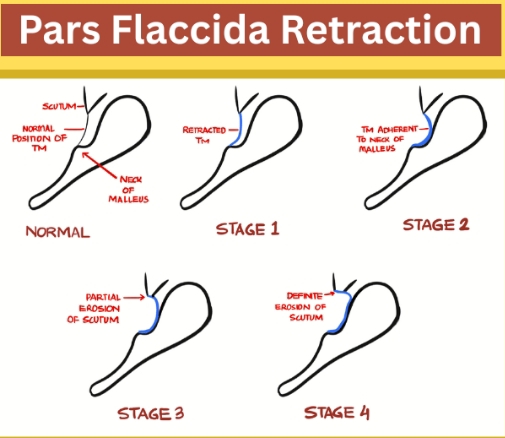
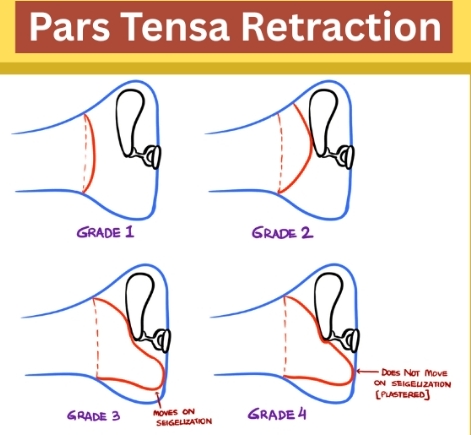
Figure 2
Sade and Tos classification for Pars retractions.
Signs & Symptoms
Symptoms of glue ear
Mainly hearing loss: “talks loudly”, turns TV up, inattentive in class. Delayed speech/language in young kids. Fullness / “popping”. Balance issues less common. Usually no pain/fever unlike acute otitis media.
Signs
Otoscopic: Dull / amber TM, reduced mobility, air-fluid level / bubbles, retraction, radial vessels. Pneumatic otoscopy shows poor / absent movement = key sign.
Investigations
Pneumatic otoscopy: Gold standard bedside test
Tympanometry: Type B, flat curve = fluid. Type C = negative pressure
Pure tone audiometry: 25-40 dB conductive loss
Nasendoscopy: If adult or suspect adenoid hypertrophy/NPC
Hearing test + speech assessment in kids
Health providers may do the following diagnosis for Otitic barotrauma:
Management
Watchful Waiting (WW) 3 months: 50% resolve spontaneously. Confirm with hearing test.
Medical management
Intranasal steroids: Minimal benefit, not routinely recommended
Autoinflation/Balloon blowing: See below
Antibiotics/Antihistamines/Decongestants: No role. Not bacterial, not allergic.
Treat comorbidities: Allergic rhinitis, reflux
Failed medical/WW after 3 months + hearing loss ≥ 25-30dB + impact: Refer ENT for surgical options
Balloon Blowing / Autoinflation
Kids blow up “Otovent balloon” via nostril 2-3x/day. Forces air up ET and equalizes pressure + pushes fluid out.
Helps especially in children:
- Improves ET function
- Reduces fluid -non-invasive.
NICE/AAO-HNS recommend trial before surgery if child >3 yrs. Works best if child can cooperate + no active infection.
Complications
Untreated Glue Ear Complications
Hearing loss: Speech delay, poor school performance
TM changes: Retraction pockets, atelectasis, cholesteatoma
Behavioral: Inattention misdiagnosed as ADHD
Balance issues: Rare
Surgical Management Complications
Grommet/Ventilation tube insertion risks:
- Otorrhea/discharge 10-20%
- Persistent perforation 1-2% after tube extrusion
Tympanosclerosis / scarring:
- Granuloma, tube blockage
- Anesthesia risks
Note on Grommets / Ventilation Tubes
Small Teflon/silicone tube placed through TM under GA. Ventilates middle ear, drains fluid. Falls out spontaneously in 6-12 months.
-
Types:
Short-term ( Shepard), and long-term ( T-tubes).
-
Indications:
Persistent OME >3-6 months + hearing loss + impact.
Submucous Cleft Palate + Grommet Endpoint
Kids with submucous cleft have poor tensor veli palatini and lifelong ET dysfunction. Endpoint: Often need repeated grommets or long-term T-tubes until palate repaired/muscle function improves. May need permanent solution. Hearing + speech development are the endpoints, not just tube extrusion.
To conclude,
Glue ear = ET dysfunction and middle ear effusion and conductive hearing loss.
Most kids resolve spontaneously. Treat comorbidities, trial autoinflation, reserve grommets for persistent cases with impact. Early detection prevents speech / learning issues.
Case Reports
Case 1: 3-year-old - Medical + Surgical Management
3yr boy, 6 months bilateral hearing loss, speech delay. Failed 3 months WW + autoinflation. Tympanometry Type B bilaterally, PTA 35dB loss. Had adenoid hypertrophy.
Management: Adenoidectomy + bilateral grommet insertion. At 6 weeks: TM clear, tympanometry Type A, speech therapy started. Hearing normalized.
Key point: Address adenoids in < 4yr olds.
Case 2: 3-year-old Down’s Syndrome
3yr girl with Down’s syndrome, recurrent OME since infancy. Poor ET function + craniofacial factors. Failed medical + 2 sets of short-term grommets. Severe language delay.
Management: Long-term T-tube grommets + aggressive speech therapy + ENT + pediatric follow-up. Required 4 sets of tubes by age 7.
Key points: Down’s kids need earlier intervention, longer tube duration, multidisciplinary rehab.
Endpoint = intelligible speech + school readiness, not just “dry ear”.
PAGE REVISION SHEET: Glue Ear / OME
- Definition
Non-infective fluid/mucus in middle ear >3mo, intact TM, no pain/fever. “Glue” = thick mucoid effusion.
- Epi
Peak 6mo-7yr. 80% kids get it by age 4. Boys > girls. Adults = rare, red flag for NPC.
- Anatomy
Kids ET = short, wide, horizontal, floppy cartilage → poor ventilation. Adults ET = long, narrow, oblique, stiff.
- Causes of ET dysfunction
URTI, adenoids, allergy, cleft palate, Down’s, barotrauma.
- Pathophysiology
ET block, neg pressure, transudate , mucus gland hyperplasia, viscous fluid and conductive hearing loss.
- Sade Grading TM retraction
G1 mild, G2 touches incus, G3 touches promontory, G4 atelectasis/adhesion.
- Symptoms
Painless hearing loss, TV loud, inattentive, speech delay. No fever.
- Signs
Dull/amber TM, bubbles/air-fluid level, reduced mobility on pneumatic otoscopy.
- Investigations
Pneumatic otoscopy + tympanometry Type B/C + PTA 25-40dB loss.
- Managements:
- WW 3 months: 50% resolve. Check hearing impact.
- Medical: Autoinflation/balloon blowing.
- Steroids / antibiotics / decongestants = no benefit.
Surgical if failed WW + ≥25 - 30dB + impact:
Grommets ± adenoidectomy.
-
Balloon blowing:
Otovent device, forces air up ET. Good for cooperative kids >3yr. NICE recommended pre-surgery.
-
Complications untreated:
Speech delay, poor school, TM retraction pockets, atelectasis, cholesteatoma.
-
Complications surgery:
Otorrhea, persistent perforation, tympanosclerosis, granuloma.
-
Grommets:
Ventilate/drain middle ear, fall out 6-12mo. Short vs long-term T-tubes.
-
Submucous cleft + grommets:
Lifelong ET dysfunction. Need repeated/long-term tubes. Endpoint = speech + hearing development, not just tube out.
Key exam points: No abx. Type B tympanogram. Pneumatic otoscopy gold standard. Adenoids matter <4yr. Down’s = early tubes + rehab.
Just quiz yourself.
Q1: What’s the difference between glue ear and AOM?
Glue ear = no pain/fever, effusion >3mo. AOM = acute infection with pain, fever, bulging TM.
Q2: Why do children get glue ear more than adults?
ET shorter, wider, more horizontal, floppy cartilage → poor ventilation / drainage.
Q3: Gold standard bedside test for OME?
Pneumatic otoscopy showing poor / absent TM mobility.
Q4: Tympanometry finding in glue ear?
Type B flat curve = fluid. Type C = negative pressure.
Q5: Sade Grade 3 retraction means?
TM retracted to touch promontory of middle ear.
Q6: 3 main functions of Eustachian Tube?
Ventilate, drain, protect middle ear from nasopharynx.
Q7: First-line management for 3mo history OME?
Watchful waiting 3 months + hearing assessment.
Q8: Do antibiotics help glue ear?
No. It’s not bacterial. Abx, antihistamines, decongestants not recommended.
Q9: How does balloon blowing help?
Forces air up ET via nose and equalizes pressure + pushes fluid out. For kids >3yr.
Q10: Indications for grommets?
OME >3-6mo + hearing loss ≥25-30dB + educational/behavioral impact.
Q11: 2 complications of untreated glue ear? n Tab Title 1
Speech delay + TM retraction/atelectasis cholesteatoma.
Q12: Main complication after grommet insertion?
Otorrhea/discharge 10-20%. Persistent perforation 1-2%.
Q13: Why are Down’s syndrome kids high risk for glue ear?
A: Poor ET muscle function + craniofacial factors and need earlier tubes + long-term T-tubes.
Q14: Endpoint for grommet management in submucous cleft palate?
Normal speech/hearing development, not just tube extrusion.
Q15: Adult with unilateral glue ear - what must you exclude?
Nasopharyngeal carcinoma. Needs nasendoscopy ± biopsy.
Share Post On:
Recent Posts
Categories
Get in Touch
Read doctor-produced health and medical information written for you to make informed decisions about your health concerns.
Address
Adenta
info@grovehealth.net
Working Hours
Mon - Friday @ 8am - 5 pm